
FFN Hypothalamic Amenorrhea Case Studies: Cycle Restoration, Fertility Outcomes, and Hormone Rebalancing
Hypothalamic amenorrhea is characterized by the loss of a menstrual cycle for six or more months. Below are two case studies from patients of ours at Functional Fueling. We outline their initial presentations, our clinical approach, and how they recovered their menstrual cycle after many years of amenorrhea. You can learn more about working with us in our 1:1 program here.
Patient 1: “Sara”
30-year-old female who established care in November 2025, one week after completing the NYC Marathon. She came in through our Functional Thyroid Foundations program looking to address ongoing fatigue, digestive issues, and loss of her menstrual cycle.
Conditions:
- Primary biliary cholangitis (PBC) (dx 2023)
- Hypothalamic amenorrhea (HA) (dx 2025)
- History of IBS-C
Symptoms:
- Chronic constipation (IBS-C), gas, bloating
- Distress after high-fat foods
- Sugar cravings, fatigue after eating, feeling shaky between meals
- Difficulty losing weight (+15 lbs during marathon training)
- Cold hands and feet, poor circulation
- Loss of menstrual cycle
- Dry, itchy skin
- Chronic fatigue (5+ years), caffeine dependency
- Poor sleep
- Feeling puffy and inflamed
Initial Clinical Strategy: Replenishment Phase
We began by focusing on calming inflammation and establishing foundational support across digestion, energy availability, and nervous system regulation. Given her diagnosis of primary biliary cholangitis (a chronic autoimmune liver condition), reducing inflammatory burden and supporting liver function were key early priorities.
Digestive support was also critical due to impaired bile flow and chronic constipation. We prioritized improving motility and opening detoxification and drainage pathways before advancing into deeper gut and immune work. This included targeted supplementation, including gut support formulas, alongside structured nutrition strategies to improve consistency and overall intake.
In complex cases involving hypothalamic amenorrhea, chronic GI dysfunction, and high training loads, restoring energy availability and physiologic stability is essential before addressing deeper hormonal and metabolic dysfunction.
Key Areas of Support
- Micronutrient repletion to support immune resilience and metabolic function
- Digestive support, bile flow optimization, and bowel regularity
- Opening detoxification and drainage pathways
- Cellular energy production and mitochondrial support
- Restoring overall energy availability through nutrition
- Nervous system and stress physiology support
- Immune modulation (given autoimmune condition and viral load)
- Gut microbiome balance and treatment of dysbiosis
- HPA and HPO axis support to restore ovarian function
Early Outcomes
- Significant improvements in overall energy
- Reduced bloating, puffiness, and inflammation
- Improved libido
- Less travel-related GI discomfort and constipation
- Increased food tolerance with fewer sensitivities
Nervous System and Immune Modulation Phase
Once foundational stability was established, care shifted toward deeper gut, immune, and nervous system support. Using a phased approach, we addressed microbial imbalances identified on prior stool testing, while continuing to support digestion, immune regulation, and metabolic function. Repeat testing was conducted to further refine treatment and address ongoing dysbiosis.
A major focus during this phase was restoring energy availability and improving hormone signaling through nutrition. Continuous glucose monitoring (CGM) was introduced and revealed that blood sugar dysregulation was being driven more by nervous system stress than food intake alone. Based on this, we adjusted exercise patterns, incorporated targeted carbohydrate increases, and implemented strategies to better support stress resilience and metabolic flexibility.
Metabolic Assessment and Optimization
Despite strong improvements in symptoms, the patient continued to experience some fatigue and difficulty with body composition, prompting deeper metabolic assessment.
Continuous glucose monitoring provided key insights:
- Impact of external stressors on blood sugar fluctuations
- Strong metabolic response to exercise
- Improved tolerance to increased carbohydrate intake
This data allowed for more targeted interventions to support metabolic efficiency, nervous system regulation, and sustainable energy production.
Clinical Outcomes
Repeat GI MAP testing showed significant improvements:
- E. coli cleared
- Reduced steatocrit (a marker of poor fat digestion)
- Optimized secretory IgA
- Reduction in anti-gliadin markers
- Identification and treatment of biofilms and remaining dysbiosis
By February, the patient began experiencing PMS-like symptoms, indicating reactivation of hormonal signaling.
By the end of February, she experienced her first full menstrual cycle in 7 years, approximately 3–4 months into care.
Patient Results
- Restoration of menstrual cycle
- Significant improvement in energy and exercise tolerance
- Reduced bloating, puffiness, and inflammation
- Improved digestive function and regularity
- Reduced stress around food choices
- Improved overall strength, resilience, and well-being
Initial Stool Test:
Repeat Stool Test 9 Months Later:
Initial Viral Infections Panel: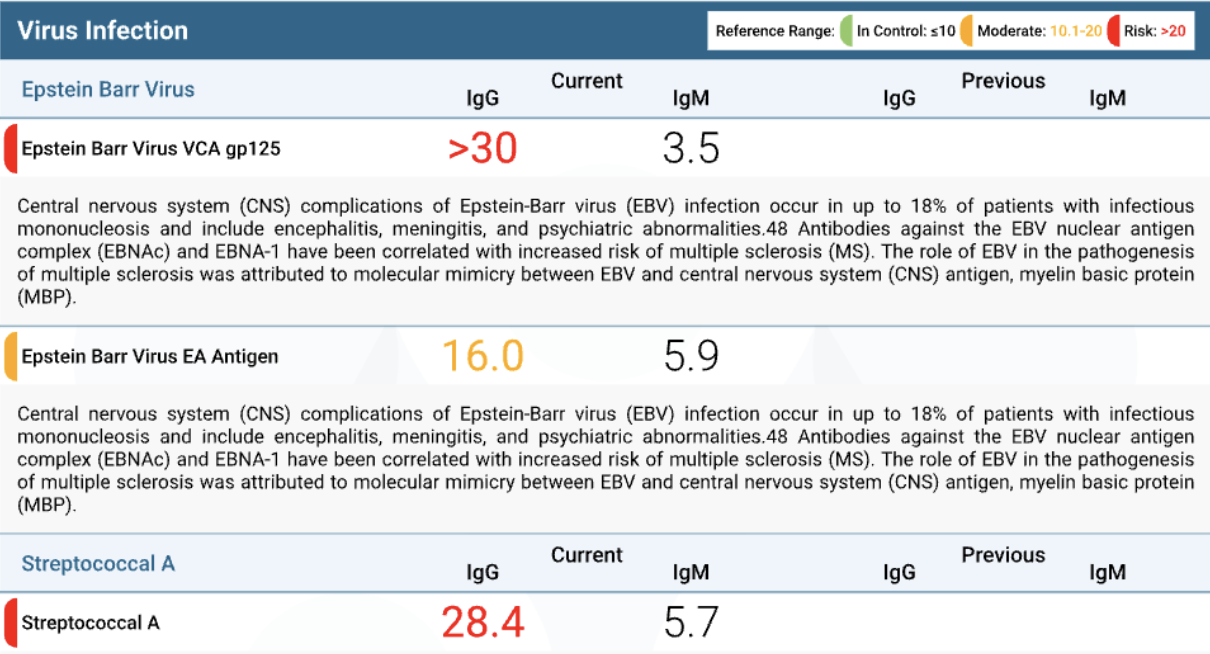
Patient 2: Jenny
The patient presented with a 4+ year history of amenorrhea and was unsure whether her symptoms were driven by hypothalamic amenorrhea (HA), PCOS, or thyroid dysfunction. She came to Functional Fueling seeking answers around her missing cycle, fertility concerns, and ongoing digestive and energy-related symptoms.
After restoring her cycle, she successfully conceived and is now in her third trimester, continuing care for a healthy pregnancy.
Conditions:
- Undiagnosed Amenorrhea (unclear etiology initially: HA vs PCOS)
- Infertility
- Subclinical hypothyroidism (on medication)
- History of IBS-C
Symptoms:
- Absent menstrual cycle (4+ years)
- Moderate fatigue and post-meal fatigue
- Sluggish digestion, bloating
- Not waking up hungry
- Occasional sleeplessness
- PMS-type symptoms and hormonal headaches
- Decreased libido
- Acne
Initial Clinical Strategy: Replenishment Phase
Care began with a strong emphasis on restoring foundational nutrition and improving overall energy availability, both critical in cases of amenorrhea. This included implementing consistent meal timing, improving meal composition, and increasing carbohydrate intake to better support metabolic and hormonal signaling.
Early support also focused on digestion and liver function, as symptoms of bloating, sluggish digestion, and IBS-C history suggested underlying gastrointestinal involvement. GI MAP testing was utilized to further assess gut health and guide targeted interventions.
Given the complexity of her presentation, early investigation focused on differentiating between hypothalamic amenorrhea, PCOS, thyroid involvement, and gut-related drivers, while prioritizing stabilization before deeper interventions.
Key Areas of Support
- Foundational nutrition and energy availability
- Meal consistency (timing and composition)
- Carbohydrate repletion to support hormone signaling
- Anti-inflammatory nutrition and oxidative stress support
- Digestive function, detoxification, and elimination pathways
- Gut microbiome treatment and repair
- Metabolic health and blood sugar regulation
- Exercise performance and recovery support
Early Outcomes
- Improved digestion and reduced bloating
- Better tolerance to dietary fats
- Reduction in stress-related gastrointestinal symptoms
- Decreased overall inflammation
Slightly later outcomes:
- More consistent energy levels
- Improved stress resilience
- Pregnancy
Nervous System and Immune Modulation Phase
As care progressed, a major focus was placed on nervous system regulation, particularly important in hypothalamic amenorrhea cases, where allostatic load plays a significant role in suppressing reproductive function. This included addressing multiple contributors to HPA axis dysregulation, such as chronic stress, under-fueling, exercise load, and underlying gut and immune factors.
During this phase, treatment required careful adjustment after an initial response to more aggressive gut and detox protocols. By scaling back to a more gentle, supportive approach, the patient stabilized quickly and experienced significant improvements.
Continuous glucose monitoring (CGM) was also introduced, revealing that blood sugar fluctuations were strongly influenced by stress and nervous system triggers rather than food alone. This provided valuable insight and allowed for more targeted metabolic and lifestyle interventions.
Within approximately 3 months of care, the patient successfully restored her menstrual cycle.
Metabolic Assessment and Optimization
Following cycle restoration, care shifted toward optimizing metabolic, hormonal, and fertility outcomes.
Strategies included:
- Ongoing gut healing and targeted mycotoxin support
- Use of at-home hormone tracking to monitor cycle patterns
- Adjustments to exercise to reduce oxidative stress
- Increased dietary antioxidants and overall nutrient density
- Improved fat intake, including saturated fats, to support hormone production
- Circadian rhythm support through strategic light exposure and travel routines
- Targeted adaptogen use for continued nervous system support
- Approximately 6 months after cycle restoration, the patient conceived.
Clinical Outcomes
- Restored menstrual cycle within 3 months working together after 4+ years of amenorrhea
- Improved digestion and reduced bloating
- Increased energy and metabolic stability
- Improved stress resilience and nervous system regulation
- Successful conception and ongoing healthy pregnancy
Patient Results
- Return of natural menstrual cycle
- Improved relationship with food and hunger cues
- Reduced digestive symptoms
- More stable energy and mood
- Healthy pregnancy and improved overall well-being
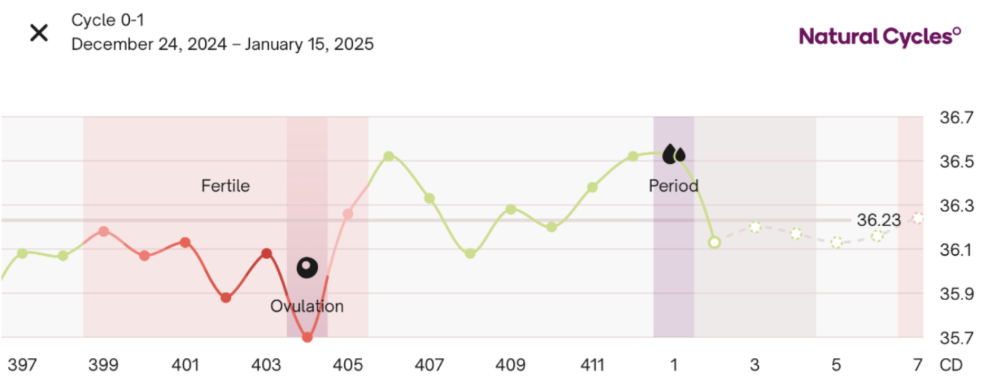
Initial Cycle Data When We Began Care:

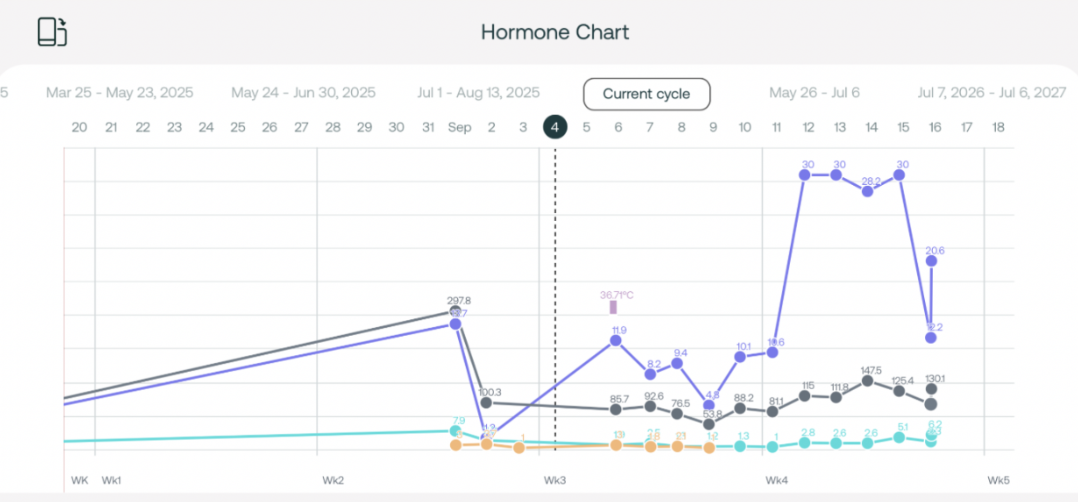
Cycle Data When Period Returned:
Cycle Data Confirming Pregnancy:
Initial Thyroid Labs:

Thyroid Labs After 1 Year:
 (*10 weeks pregnant)
(*10 weeks pregnant)
As shown above, her FT3 increased from 2.2 pg/mL to 2.73 pg/mL over the course of one year.
Get to the Root of your Hypothalamic Amenorrhea
Amenorrhea is rarely just about your cycle, it’s often a reflection of deeper disruptions in energy availability, thyroid function, and immune balance.
We specialize in working with individuals navigating complex, overlapping conditions to uncover the true drivers and build a clear, personalized path forward.
→ Start with our Low T3 Quiz to understand what may be driving your symptoms
")

Comments +